Ruxolitinib for vitiligo: what clinical studies really say
A necessary premise
In 2022, topical ruxolitinib (Opzelura®) was approved by the FDA, EMA, and subsequently AIFA as the first treatment specifically indicated for vitiligo. Its approval generated great enthusiasm in the scientific community and the media, because for the first time a drug was presented as a “causal” treatment for the disease.
This interest led to awareness campaigns, public initiatives, and extensive media coverage. However, when analyzing the clinical data published in the registration studies, the picture appears more complex than the often simplified narrative suggests.
This article analyzes the results of clinical studies on ruxolitinib in vitiligo with an approach based on the available scientific data and on the clinical experience gained by the Dermacademy Institute in managing the disease.

What ruxolitinib is and how it works
Ruxolitinib is a drug belonging to the class of Janus kinase inhibitors (JAK1 and JAK2), enzymes involved in transmitting inflammatory signals within cells.
In vitiligo, the immune system activates an autoimmune response mediated by T lymphocytes, leading to the destruction of melanocytes, the cells responsible for melanin production.
By blocking the JAK-STAT pathway, ruxolitinib reduces the activation of inflammatory signals that contribute to the loss of melanocytes in the skin.
The drug exists in two main formulations:
-
oral, used for hematological diseases such as myelofibrosis and polycythemia vera
-
topical 1.5% cream, approved for vitiligo and atopic dermatitis
The biological rationale of the drug is solid. The clinical discussion mainly concerns the real effectiveness observed in clinical studies.
What phase 3 studies say
The approval of topical ruxolitinib is based on two randomized phase 3 clinical studies, conducted on 674 patients with bilateral vitiligo.
The primary endpoint used in the studies is F-VASI75, meaning the percentage of patients achieving at least 75% repigmentation of facial patches.
Results on the face
The main results show:
| Time | Ruxolitinib | Placebo |
|---|---|---|
| 6 months | 28.2% | 11.2% |
| 12 months | 50.2% | not available |
After six months of treatment, fewer than three out of ten patients achieve significant facial repigmentation. After twelve months of twice-daily application, approximately half of patients achieve this result.
These are clinically relevant data, but they must be interpreted within the context of the available therapeutic alternatives.

Comparison with other topical treatments
One often under-discussed element concerns the comparison with other drugs already used in vitiligo.
A randomized multicenter study on topical tacrolimus 0.1% showed different results for the same clinical endpoint:
| Drug | F-VASI75 at 3 months | F-VASI75 at 6 months | Application |
|---|---|---|---|
| Tacrolimus 0.1% | 50% | 65% | once daily |
| Ruxolitinib 1.5% | not reported | 28.2% | twice daily |
In this study, tacrolimus achieved in three months a result comparable to that observed with ruxolitinib after longer treatment periods.
This comparison does not indicate that one drug is universally superior to the other, but shows how the evaluation of therapies must always consider:
-
clinical effectiveness
-
response times
-
method of application
-
cost of treatment.
Results on the body
While data on the face show a certain degree of effectiveness, results on other areas of the body are more limited.
In clinical studies, the initial endpoint for the body was T-VASI75, meaning 75% repigmentation of total patches.
After six months of treatment:
-
only 11.2% of patients achieved this result.
For this reason, in the subsequent phases of the studies, the endpoint was changed to T-VASI50, a lower improvement threshold.
From a clinical perspective, this means that for many patients with extensive body vitiligo, the results of topical ruxolitinib alone may be limited.
Side effects of topical ruxolitinib
In phase 3 studies, approximately 50% of patients reported at least one side effect during treatment.
The most common effects include:
-
acne in the application area
-
itching
-
nasopharyngitis or rhinitis
-
headache
-
urinary tract infections.
These reactions are generally manageable, but the overall rate of adverse events is relatively high for a topical treatment.
Long-term safety: what we know
One frequently discussed topic concerns the long-term safety of drugs that act on the JAK pathway.
A study published in 2024 in the journal Blood analyzed patients with myelofibrosis treated with oral ruxolitinib over prolonged periods. The results showed:
-
12 deaths from metastatic non-melanoma skin cancers
-
11 deaths due to progression of myelofibrosis.
It is important to emphasize that:
-
the study concerns the oral formulation, with much higher systemic doses
-
the patients were already affected by serious hematological diseases.
These data cannot be automatically transferred to topical ruxolitinib, but they suggest the need for careful dermatological monitoring during prolonged treatments.
The cost of treatment
Another element to consider is the cost of the drug.
Topical ruxolitinib has an indicative price of approximately €1,200 for 100 grams of cream.
In Italy, it may be dispensed by the National Health Service through a therapeutic plan, but the cost for the healthcare system remains high.
In addition to the direct economic cost, there is also an indirect clinical cost: time spent on a poorly effective treatment may delay the start of more appropriate therapeutic strategies.
Ruxolitinib and vitiligo treatment: a clinical perspective
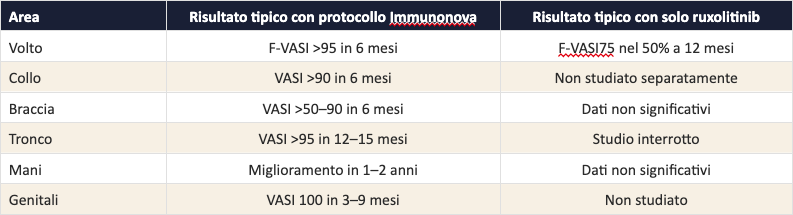
Topical ruxolitinib is a drug with a coherent biological mechanism and demonstrated effectiveness especially for facial patches.
However, the available data also show some limitations:
-
variable effectiveness among patients
-
more modest results on body areas
-
non-negligible side effects
-
high costs.
Vitiligo is a complex and systemic autoimmune disease. For this reason, many clinical approaches today integrate different therapeutic tools instead of relying on a single topical treatment.
Conclusion: reading the data carefully
The approval of ruxolitinib represented an important step in vitiligo research. However, a complete clinical evaluation always requires analyzing the scientific data as a whole.
Patients have the right to know:
-
the real benefits of a treatment
-
its limitations
-
the possible therapeutic alternatives.
Managing vitiligo often requires a broader approach, based on clinical evaluation, monitoring over time, and personalized therapeutic strategies.
Are you using ruxolitinib for vitiligo and not seeing results?
A specialist evaluation can help understand the activity of the disease and define a therapeutic pathway better suited to your case.
Discover which clinical strategies are used today to address vitiligo comprehensively.
Author: Dr. Giovanni Menchini